Bladder Cancer: Symptoms, Types, Treatment & Prevention (2026 Complete Guide)
Bladder Cancer: Symptoms, Types, Treatment & Prevention (2026 Complete Guide)
Published: January 2026 | Medical Review: This guide has been updated with the latest 2025-2026 clinical guidelines and research findings from leading urology and oncology sources.
Bladder cancer is the 6th most common cancer in the United States, with approximately 83,000 new cases diagnosed annually in 2025. This comprehensive 2026 guide breaks down everything you need to know—from early warning signs and types to modern treatment options and prevention strategies—helping patients and families navigate diagnosis and beyond with greater clarity.
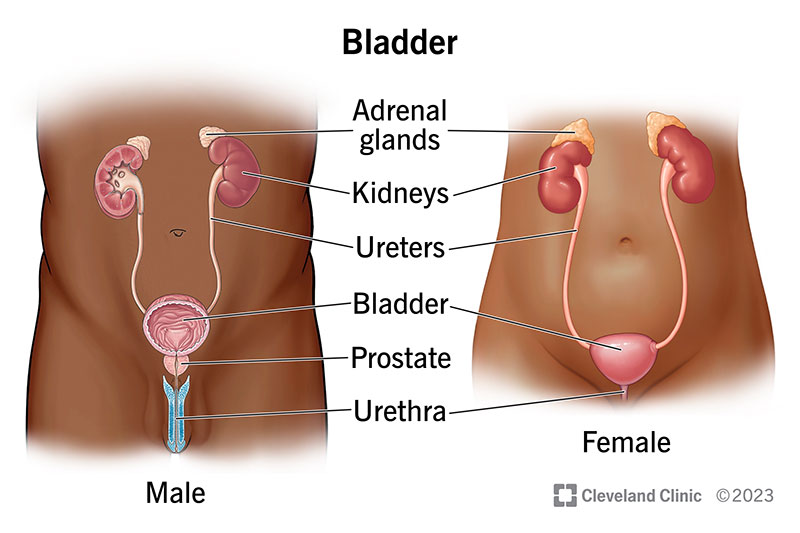
Anatomy of the human bladder (Source: Cleveland Clinic)

Overview infographic of bladder cancer (symptoms, types, and more)
Understanding Bladder Cancer: The Basics
Bladder cancer is the uncontrolled growth of abnormal cells in the urothelium, the lining of the bladder. The bladder is a hollow, muscular organ in the pelvis that stores urine. Most bladder cancers (about 90%) are urothelial carcinomas (also called transitional cell carcinomas), which start in the urothelial cells lining the bladder's interior.
Key Statistics at a Glance (2026 Data)
- Annual New Cases (U.S.): ~83,000 (estimated for 2025)
- Annual Deaths (U.S.): ~16,500 (showing slight decline due to earlier detection)
- Gender Disparity: 3-4 times more common in men (Lifetime risk: 1 in 26 for men, 1 in 84 for women)
- Average Age at Diagnosis: 73 years
- #1 Preventable Risk Factor: Smoking (triples the risk)
- Global Impact: 10th most common cancer worldwide
Recognizing the Symptoms and Early Signs
Early symptoms can be mistaken for less serious conditions like a urinary tract infection (UTI). Knowing the signs leads to earlier diagnosis and significantly better outcomes.
The most common and often first symptom is hematuria, or blood in the urine. It may be:
- Gross hematuria: Visible, making urine appear pink, red, or cola-colored.
- Microscopic hematuria: Only detectable under a microscope during a urinalysis.
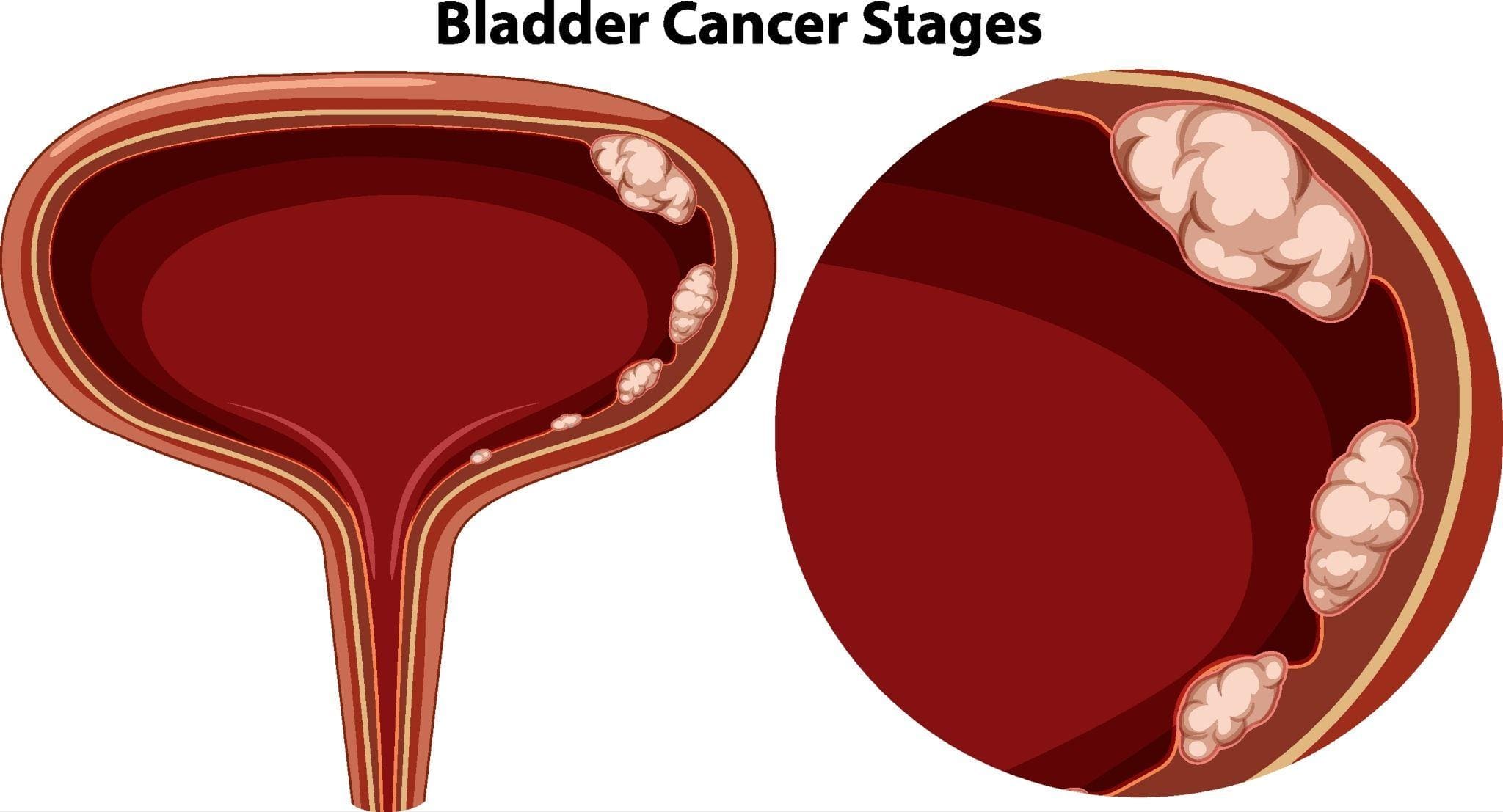
Illustration showing blood in urine (hematuria), a key symptom of bladder cancer
Other symptoms can include:
- Frequent urination
- Pain or a burning sensation during urination (dysuria)
- Feeling an urgent need to urinate
- Feeling the need to urinate without results
- Pelvic or back pain (especially in advanced stages)
- Unexplained weight loss and fatigue (in metastatic disease)
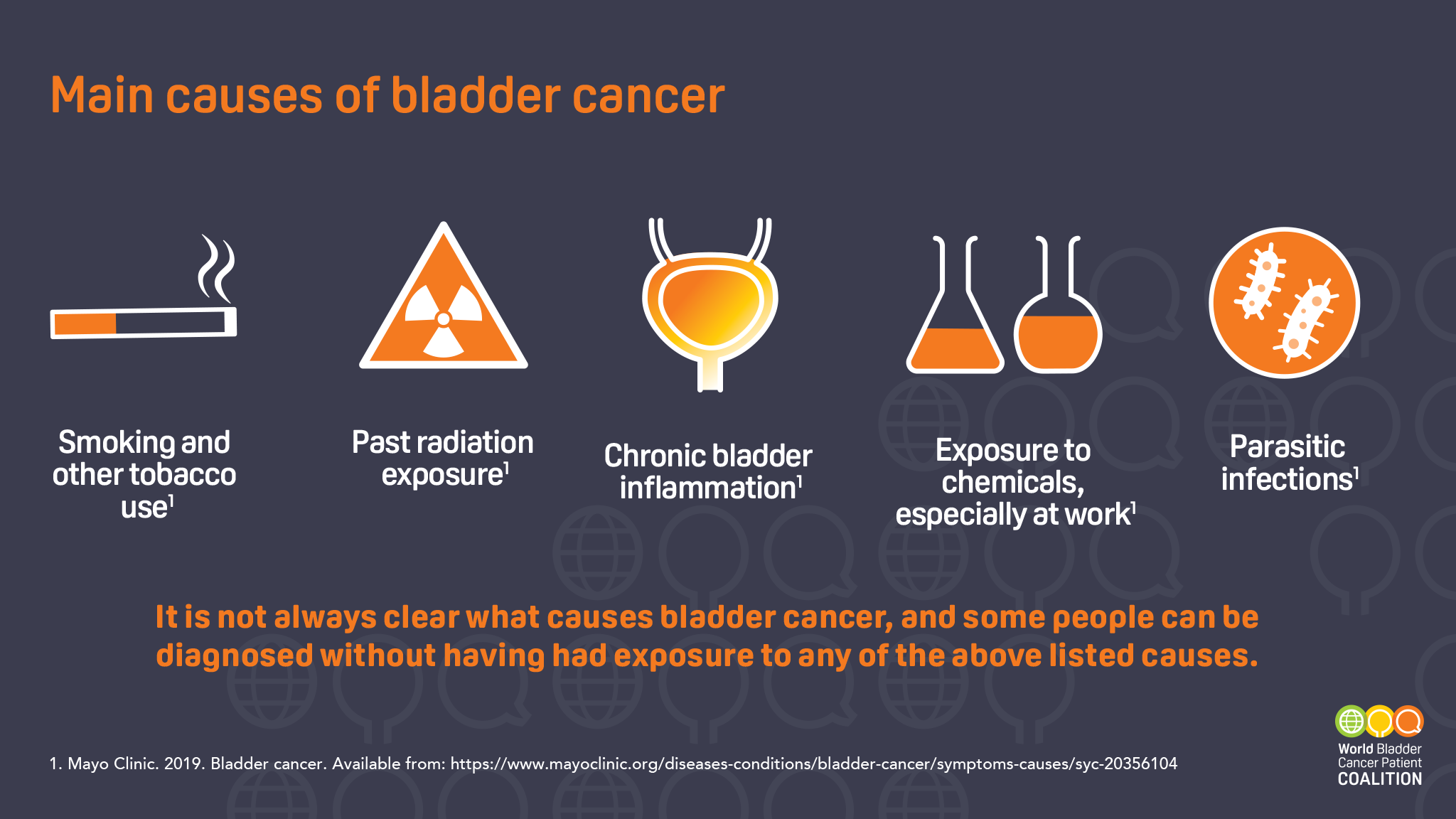
What Causes Bladder Cancer? Key Risk Factors
Understanding risk factors aids in prevention and proactive health monitoring.
Infographic of key bladder cancer risk factors, including smoking and chemical exposure
Primary Risk Factors Include:
- Smoking: The single greatest preventable risk. Harmful chemicals are filtered by the kidneys and concentrate in urine, damaging bladder lining. E-cigarettes/vaping are now also considered risk factors.
- Chemical Exposure: Occupational exposure to aromatic amines (used in dye, rubber, paint industries).
- Age & Gender: Risk increases with age; men are disproportionately affected.
- Chronic Bladder Irritation: From long-term catheter use or recurrent infections.
- Personal/Family History: Previous bladder cancer or family history of Lynch syndrome.
- Prior Radiation Therapy: Especially to the pelvic region.
- Arsenic in Drinking Water: Particularly in certain geographical areas.
- Certain Medications: Long-term use of pioglitazone for diabetes.
Types and Staging: From NMIBC to MIBC
Accurate classification is vital as it dictates treatment.
Main Types of Bladder Cancer
| Type | Description | Prevalence |
|---|---|---|
| Urothelial Carcinoma | Begins in urothelial cells lining the bladder. | ~90% |
| Squamous Cell Carcinoma | Associated with chronic bladder irritation/infection. | 1-2% (U.S.) |
| Adenocarcinoma | Develops from glandular cells; very rare. | <1% |
| Small Cell Carcinoma | Rare, aggressive neuroendocrine tumor. | <1% |
| Sarcomatoid Variant RARE | Highly aggressive variant with spindle cells. | <1% |
The Critical Distinction: NMIBC vs. MIBC
The most important determination is whether cancer has invaded the muscle layer of the bladder wall.
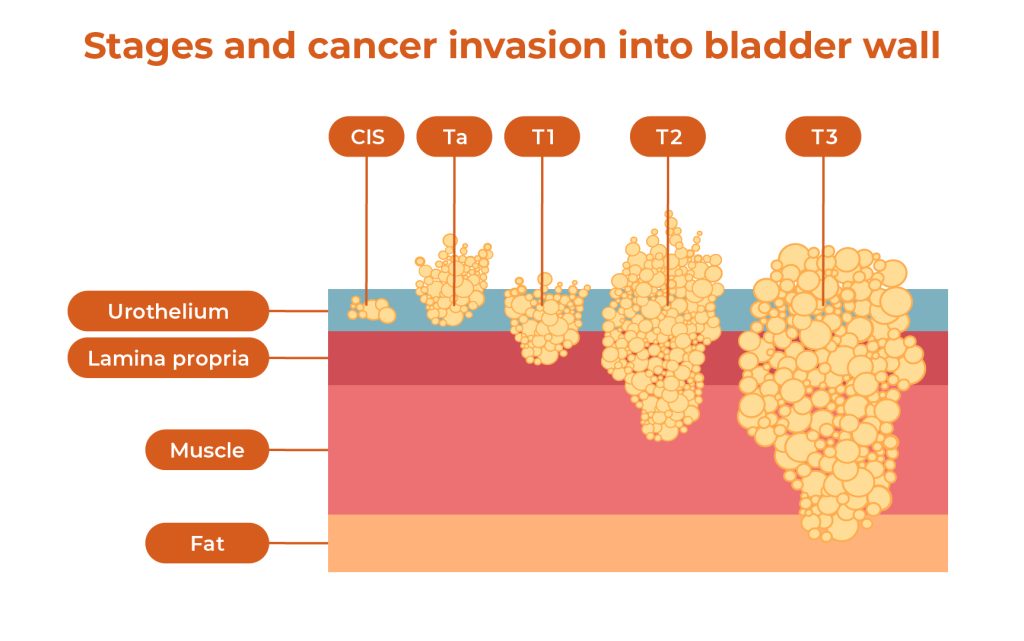
Diagram illustrating non-muscle-invasive vs. muscle-invasive bladder cancer stages
| Feature | Non-Muscle-Invasive (NMIBC) | Muscle-Invasive (MIBC) |
|---|---|---|
| Prevalence at Diagnosis | ~75% of cases | ~25% of cases |
| Depth of Invasion | Inner lining (mucosa) or connective tissue only. | Invades the muscle layer. |
| Metastasis Risk | Low | High |
| Primary Treatment | TURBT + Intravesical Therapy (e.g., BCG) | Radical cystectomy or trimodal therapy |
| 5-Year Survival | Over 90% for Stage 0 | ~70% for localized MIBC |
| 2026 Update | New risk stratification models incorporating molecular markers | Increased use of neoadjuvant immunotherapy combinations |
📊 For a complete visual breakdown of what each stage means, see our detailed guide on Bladder Cancer Stages.
The Diagnosis Process: Step-by-Step
Diagnosis typically follows a structured pathway:

Illustration of cystoscopy, a key diagnostic procedure for bladder cancer
- Initial Evaluation & Urine Tests: Includes medical history, physical exam, urinalysis, and urine cytology to look for cancer cells. New in 2026: Urine-based biomarker tests (like UroSEEK, Cxbladder) are increasingly used as adjuncts.
- Cystoscopy: The cornerstone procedure. A urologist inserts a thin, lighted tube (cystoscope) through the urethra to view the bladder lining directly and biopsy any suspicious areas. Blue-light cystoscopy with HALO is now standard for improved detection.
- Imaging: A CT urogram or MRI is used to check the upper urinary tracts (kidneys, ureters) and see if cancer has spread. PET/CT is increasingly used for staging MIBC.
- TURBT (Transurethral Resection of Bladder Tumor): This is both the definitive diagnostic and initial treatment procedure for NMIBC. The tumor is removed and analyzed to determine its type, grade, and precise stage. Molecular profiling is now often performed.
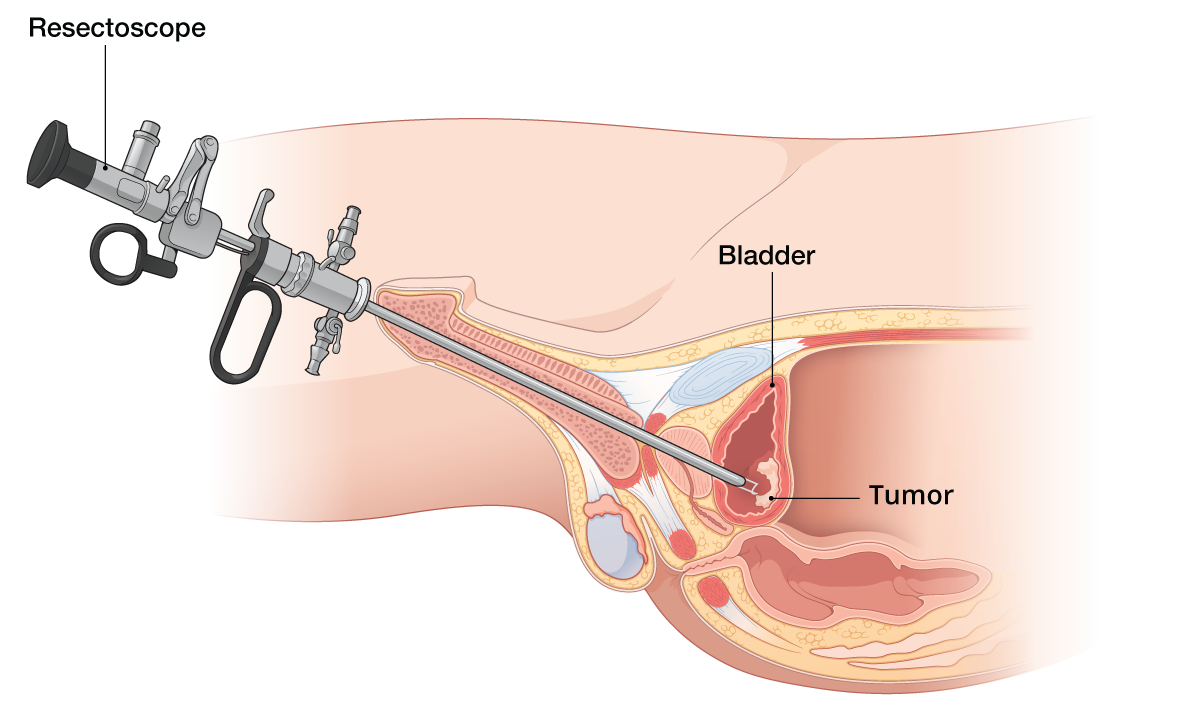
Diagram of Transurethral Resection of Bladder Tumor (TURBT)
Treatment Options by Stage (2026 Updates)
Treatment is highly personalized based on stage, grade, molecular profile, and overall health.
For Non-Muscle-Invasive Bladder Cancer (NMIBC)
- TURBT: The initial surgical removal of the tumor. En-bloc resection techniques are becoming more common.
- Intravesical Therapy: Medication delivered directly into the bladder via a catheter to kill remaining cells and prevent recurrence.
- Immunotherapy (BCG): A weakened bacteria that stimulates an immune response against cancer cells. It's the most effective treatment for high-risk NMIBC. BCG shortage mitigation: Alternative regimens and new agents are being used.
- Chemotherapy: Drugs like mitomycin C or gemcitabine are used to kill cancer cells.
- New Options: Nadofaragene firadenovec (Adstiladrin®) gene therapy for BCG-unresponsive CIS.
- Radical Cystectomy: Considered for highest-risk NMIBC that progresses despite intravesical therapy.
:max_bytes(150000):strip_icc()/bcg-immunotherapy-4843201-ADD-FINAL-V32-7ca128db117246f3a41ebb41acc9abf7.png)
Illustration of BCG immunotherapy delivery into the bladder
Comparing Common Intravesical Therapies:
| Aspect | BCG Immunotherapy | Intravesical Chemotherapy | Newer Agents (2026) |
|---|---|---|---|
| Primary Use | High-risk NMIBC, carcinoma in situ (CIS) | Intermediate-risk NMIBC, after TURBT | BCG-unresponsive disease |
| How it Works | Stimulates the body's immune system | Directly kills cancer cells | Gene therapy, targeted delivery |
| Common Side Effects | Flu-like symptoms, bladder irritation, blood in urine | Bladder irritation, urinary frequency | Varies by agent |
| Typical Schedule | Weekly for 6 weeks, then maintenance | Often a single dose post-TURBT or weekly | Every 3 months (e.g., Adstiladrin) |
For Muscle-Invasive Bladder Cancer (MIBC)
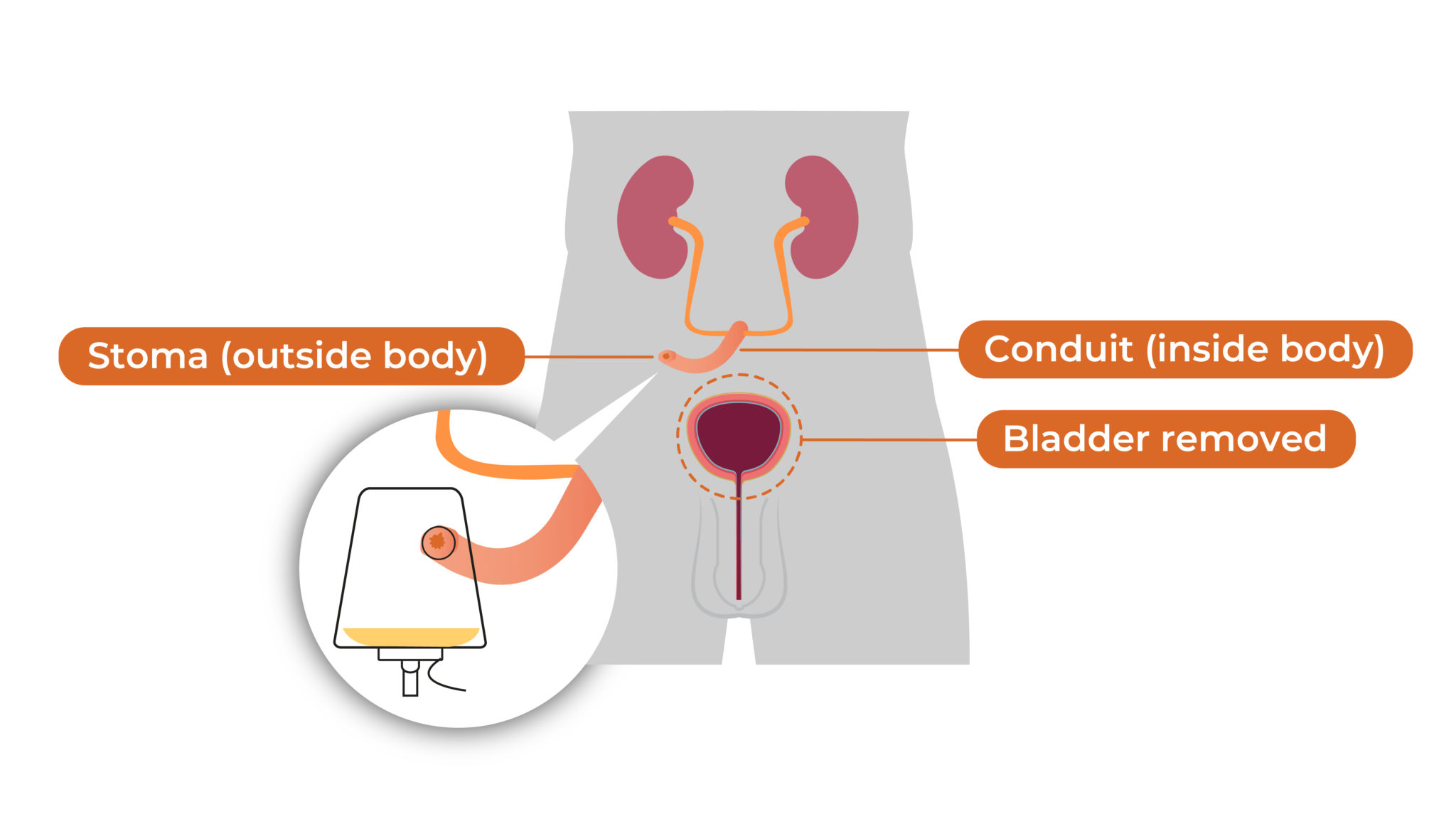
Diagram of radical cystectomy with urinary diversion
- Neoadjuvant Therapy: STANDARD Combination chemotherapy (ddMVAC or GC) remains standard. Immunotherapy combinations (chemo + checkpoint inhibitors) are showing promise in clinical trials.
- Radical Cystectomy: Surgical removal of the entire bladder and nearby lymph nodes. Robotic-assisted surgery is now standard of care, offering faster recovery. Nerve-sparing techniques improve quality of life.
- Trimodal Therapy (Bladder Preservation): An alternative for select patients, combining a maximal TURBT, radiation therapy, and chemotherapy. Success rates have improved with better patient selection and techniques.
- Systemic Therapy for Advanced/Metastatic:
- Immunotherapy: Checkpoint inhibitors (pembrolizumab, atezolizumab) as 1st/2nd line.
- Antibody-Drug Conjugates: Enfortumab vedotin (Padcev®) + pembrolizumab is now 1st line for metastatic disease.
- Targeted Therapy: Erdafitinib for FGFR-altered tumors.
- Chemotherapy: Still used, especially in combination regimens.
Life After Diagnosis: Survival Rates and Follow-Up
Prognosis varies greatly by stage at diagnosis, with improvements seen across all stages due to better treatments.

Infographic showing bladder cancer survival rates by stage
5-Year Relative Survival Rates (Latest SEER Data):
- In Situ (non-invasive): 96%
- Localized (confined to bladder): 71%
- Regional (spread to nearby tissues/lymph nodes): 39%
- Distant (metastasized): 8%
- All Stages Combined: 77% (improving due to earlier detection)
Life After Treatment: The Follow-Up Schedule
Consistent monitoring is crucial, especially for NMIBC with high recurrence rates. A typical schedule may include:
- First 2 Years: Cystoscopy and urine cytology every 3-6 months. Urine biomarker testing may be used.
- Years 3-5: Exams every 6-12 months.
- Beyond 5 Years: Annual monitoring for some patients.
- For MIBC: Regular imaging (CT scans) in addition to cystoscopy.
Prevention and Risk Reduction Strategies
Prevention strategies for reducing bladder cancer risk
While not all cases are preventable, you can significantly reduce risk:
- Do Not Smoke: This is the most effective action. If you smoke, quitting reduces risk by 40% within 1-4 years.
- Limit Chemical Exposure: Follow workplace safety protocols if working with carcinogens.
- Stay Hydrated: Drinking plenty of fluids may dilute potential carcinogens in urine.
- Eat a Balanced Diet: Focus on fruits and vegetables; cruciferous vegetables (broccoli, cabbage) may be particularly protective.
- Manage Chronic Infections: Treat UTIs and schistosomiasis promptly.
- Know Your Family History: Genetic counseling if Lynch syndrome or other hereditary patterns.
- Screen If High Risk: Annual urinalysis for those with significant occupational exposure or strong family history.
Frequently Asked Questions (FAQ) - 2026 Updates
What is the first sign of bladder cancer?
The most common first sign is painless blood in the urine (hematuria), which may come and go. Even a single episode warrants medical evaluation with cystoscopy.
Is bladder cancer curable?
Yes, especially when caught early. The 5-year survival rate for localized, non-muscle-invasive bladder cancer is over 90%. Even muscle-invasive disease can often be cured with aggressive treatment. New systemic therapies are improving curability for some advanced cases.
What are the newest treatments for bladder cancer in 2026?
The field is advancing rapidly. Key developments include:
- Antibody-drug conjugate combinations: Enfortumab vedotin + pembrolizumab as new 1st line for metastatic disease
- Intravesical gene therapy: Nadofaragene firadenovec for BCG-unresponsive CIS
- Improved bladder preservation: Better patient selection and radiation techniques for trimodal therapy
- Personalized neoadjuvant therapy: Biomarker-driven approaches in clinical trials
- Next-generation immunotherapy: Novel checkpoint inhibitors and combination regimens
How often does bladder cancer come back?
Recurrence is common with NMIBC, with rates ranging from 30-80% depending on risk factors. This is why long-term, rigorous follow-up with cystoscopy is a standard part of care. New risk stratification tools help predict recurrence likelihood.
What's being done about the BCG shortage?
The global BCG shortage continues in 2026. Mitigation strategies include:
- Reduced-dose or alternative schedule regimens
- Use of intravesical chemotherapy for intermediate-risk patients
- Approval of new agents (like gene therapy) for BCG-unresponsive disease
- Increased manufacturing capacity (long-term solution)
Disclaimer: This 2026 guide is for informational purposes only and does not constitute medical advice. Treatment guidelines evolve rapidly. Always consult with a qualified healthcare professional, such as a urologist or oncologist, for diagnosis, treatment decisions, and personalized medical care based on the latest evidence.
🔬 Stay Updated: Bladder cancer research is advancing quickly. For the latest clinical trial information and treatment breakthroughs, visit the National Cancer Institute or Bladder Cancer Advocacy Network.



Comments
Post a Comment